Does Calcaneal Apophysitis Often Have To Have Surgical Treatment?
Overview
Sever?s Disease is often misdiagnosed as a simple growing pains and affects boys far more often than girls, especially between the ages of 8 and 14. It is extremely common in children that play Soccer, Basketball, And Hockey. However it is not limited to these sports alone, nor is it simply a pre-season type condition related to fitness. Sever?s Disease sounds terrible, but there is no need to panic as it is not a contagious or incurable condition. In children, there is a growth plate in the heel bone, which at puberty becomes solid and forms part of the heel, however prior to puberty it can cause pain if the child?s foot rolls inwards or outwards too much, causing increased stress on this growth plate and inturn causes pain.
Causes
Your child?s heel bone keeps forming new bone until the late teens. The new bone is weak and can be damaged by running or pounding on hard surfaces, like during a basketball game. The new bone may also be irritated by shoes with poor padding in the heels or poor arch supports.
Symptoms
The typical patient is a child between 10 and 13 years of age, complaining of pain in one or both heels with running and walking. The pain is localized to the point of the heel where the tendo-Achilles inserts into the calcaneus, and is tender to deep pressure at that site. Walking on his toes relieves the pain.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
Podiatrists have an important role in the provision of orthotics to young sufferers of Severs? disease. Orthotics are specialised insoles designed to accommodate problems with the foot. In this particular condition?s case, orthotics are an effective way of making sure that the heel is cushioned in such a way as to reduce a child?s discomfort and alleviate some of the pressure of walking, thereby facilitating the recovery process. Young athletes can benefit from a visit to a podiatrist to learn about prevention and to have orthotics fitted to prevent Severs? disease from developing. Regular stretching to keep joints supple and loose are a great preventative measure, as is making sure that appropriately fitted and supportive shoes (often equipped with orthotics) are used to prevent future injury.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever?s Disease is often misdiagnosed as a simple growing pains and affects boys far more often than girls, especially between the ages of 8 and 14. It is extremely common in children that play Soccer, Basketball, And Hockey. However it is not limited to these sports alone, nor is it simply a pre-season type condition related to fitness. Sever?s Disease sounds terrible, but there is no need to panic as it is not a contagious or incurable condition. In children, there is a growth plate in the heel bone, which at puberty becomes solid and forms part of the heel, however prior to puberty it can cause pain if the child?s foot rolls inwards or outwards too much, causing increased stress on this growth plate and inturn causes pain.
Causes
Your child?s heel bone keeps forming new bone until the late teens. The new bone is weak and can be damaged by running or pounding on hard surfaces, like during a basketball game. The new bone may also be irritated by shoes with poor padding in the heels or poor arch supports.
Symptoms
The typical patient is a child between 10 and 13 years of age, complaining of pain in one or both heels with running and walking. The pain is localized to the point of the heel where the tendo-Achilles inserts into the calcaneus, and is tender to deep pressure at that site. Walking on his toes relieves the pain.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
Podiatrists have an important role in the provision of orthotics to young sufferers of Severs? disease. Orthotics are specialised insoles designed to accommodate problems with the foot. In this particular condition?s case, orthotics are an effective way of making sure that the heel is cushioned in such a way as to reduce a child?s discomfort and alleviate some of the pressure of walking, thereby facilitating the recovery process. Young athletes can benefit from a visit to a podiatrist to learn about prevention and to have orthotics fitted to prevent Severs? disease from developing. Regular stretching to keep joints supple and loose are a great preventative measure, as is making sure that appropriately fitted and supportive shoes (often equipped with orthotics) are used to prevent future injury.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Treatment Of Acquired Flat Foot
Overview
Adult-Acquired Flat Foot Deformity (AAFFD) is most commonly caused by a progressive degeneration of the tendon (tibialis posterior) that supports the arch of the foot. As the tendon ages or is subjected to repetitive trauma, it stretches out over time, the natural arch of the foot becomes less pronounced and the foot gradually flattens out. Although it is uncertain why this occurs, the problem is seen equally among men and women - at an increasing frequency with age. Occasionally, a patient will experience a traumatic form of the condition as a result of a fall from a height or abnormal landing during aerial sports such as gymnastics or basketball. 
Causes
A person with flat feet has greater load placed on the posterior tibial tendon which is the main tendon unit supporting up the arch of the foot. Throughout life, aging leads to decreased strength of muscles, tendons and ligaments. The blood supply diminishes to tendons with aging as arteries narrow. Heavier, obese patients have more weight on the arch and have greater narrowing of arteries due to atherosclerosis. In some people, the posterior tibial tendon finally gives out or tears. This is not a sudden event in most cases. Rather, it is a slow, gradual stretching followed by inflammation and degeneration of the tendon. Once the posterior tibial tendon stretches, the ligaments of the arch stretch and tear. The bones of the arch then move out of position with body weight pressing down from above. The foot rotates inward at the ankle in a movement called pronation. The arch appears collapsed, and the heel bone is tilted to the inside. The deformity can progress until the foot literally dislocates outward from under the ankle joint.
Symptoms
PTTD begins with a gradual stretching and loss of strength of the posterior tibial tendon which is the most important tendon supporting the arch of the human foot. Left untreated, this tendon will continue to lengthen and eventually rupture, leading to a progressive visible collapse of the arch of the foot. In the early stages, patients with PTTD will notice a pain and swelling along the inner ankle and arch. Many times, they are diagnosed with ?tendonitis? of the inner ankle. If the foot and ankle are not properly supported during this early phase, the posterior tibial tendon can rupture and devastating consequences will occur to the foot and ankle structure. The progressive adult acquired flatfoot deformity will cause the heel to roll inward in a ?valgus? or pronated direction while the forefoot will rotate outward causing a ?duckfooted? walking pattern. Eventually, significant arthritis can occur in the joints of the foot, the ankle and even the knee. Early diagnosis and treatment is critical so if you have noticed that one, or both, of your feet has become flatter in recent times come in and have it checked out.
Diagnosis
First, both feet should be examined with the patient standing and the entire lower extremity visible. The foot should be inspected from above as well as from behind the patient, as valgus angulation of the hindfoot is best appreciated when the foot is viewed from behind. Johnson described the so-called more-toes sign: with more advanced deformity and abduction of the forefoot, more of the lateral toes become visible when the foot is viewed from behind. The single-limb heel-rise test is an excellent determinant of the function of the posterior tibial tendon. The patient is asked to attempt to rise onto the ball of one foot while the other foot is suspended off the floor. Under normal circumstances, the posterior tibial muscle, which inverts and stabilizes the hindfoot, is activated as the patient begins to rise onto the forefoot. The gastrocnemius-soleus muscle group then elevates the calcaneus, and the heel-rise is accomplished. With dysfunction of the posterior tibial tendon, however, inversion of the heel is weak, and either the heel remains in valgus or the patient is unable to rise onto the forefoot. If the patient can do a single-limb heel-rise, the limb may be stressed further by asking the patient to perform this maneuver repetitively.
Non surgical Treatment
A painless flatfoot that does not hinder your ability to walk or wear shoes requires no special treatment or orthotic device. Other treatment options depend on the cause and progression of the flatfoot. Conservative treatment options include making shoe modifications. Using orthotic devices such as arch supports and custom-made orthoses. Taking nonsteroidal anti-inflammatory drugs such as ibuprofen to relieve pain. Using a short-leg walking cast or wearing a brace. Injecting a corticosteroid into the joint to relieve pain. Rest and ice. Physical therapy. In some cases, surgery may be needed to correct the problem. Surgical procedures can help reduce pain and improve bone alignment. 
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Do You Really Understand Heel Ache?
Overview

When walking, your heels repeatedly hit the ground with considerable force. They have to be able to absorb the impact and provide a firm support for the weight of the body. When pain develops in the heel, it can be very disabling, making every step a problem, affecting your posture. There are various types of heel Heel Pain. Some of the most common are heel spurs (plantar fasciitis); heel bursitis and heel bumps.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
See your doctor as soon as possible if you experience severe pain accompanied by swelling near your heel. There is numbness or tingling in the heel, as well as pain and fever. There is pain in your heel as well as fever. You are unable to walk normally. You cannot bend your foot downwards. You cannot stand with the backs of the feet raised (you cannot rise onto your toes). You should arrange to see a doctor if the heel pain has persisted for more than one week. There is still heel pain when you are not standing or walking.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
If you have experienced painful heels try wearing your shoes around your house in the evening. Don't wear slippers or socks or go barefoot. You may also try gentle calf stretches for 20 to 30 seconds on each leg. This is best done barefoot, leaning forward towards a wall with one foot forward and one foot back. If the pain persists longer than one month, you should visit a podiatrist for evaluation and treatment. Your feet should not hurt, and professional podiatric care may be required to help relieve your discomfort. If you have not exercised in a long time, consult your podiatric physician before starting a new exercise program. Begin an exercise program slowly. Don't go too far or too fast. Purchase and maintain good shoes and replace them regularly. Stretch each foot and achilles tendon before and after exercise. Avoid uneven walking surfaces or stepping on rocks as much as possible. Avoid going barefoot on hard surfaces. Vary the incline on a treadmill during exercise. Nobody walks uphill all the time. If it hurts, stop. Don't try to "work through the pain." Your podiatric physician/surgeon has been trained specifically and extensively in the diagnosis and treatment of all manner of foot conditions. This training encompasses all of the intricately related systems and structures of the foot and lower leg including neurological, circulatory, skin, and the musculoskeletal system, which includes bones, joints, ligaments, tendons, muscles, and nerves.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Prevention

Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities.
When walking, your heels repeatedly hit the ground with considerable force. They have to be able to absorb the impact and provide a firm support for the weight of the body. When pain develops in the heel, it can be very disabling, making every step a problem, affecting your posture. There are various types of heel Heel Pain. Some of the most common are heel spurs (plantar fasciitis); heel bursitis and heel bumps.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
See your doctor as soon as possible if you experience severe pain accompanied by swelling near your heel. There is numbness or tingling in the heel, as well as pain and fever. There is pain in your heel as well as fever. You are unable to walk normally. You cannot bend your foot downwards. You cannot stand with the backs of the feet raised (you cannot rise onto your toes). You should arrange to see a doctor if the heel pain has persisted for more than one week. There is still heel pain when you are not standing or walking.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
If you have experienced painful heels try wearing your shoes around your house in the evening. Don't wear slippers or socks or go barefoot. You may also try gentle calf stretches for 20 to 30 seconds on each leg. This is best done barefoot, leaning forward towards a wall with one foot forward and one foot back. If the pain persists longer than one month, you should visit a podiatrist for evaluation and treatment. Your feet should not hurt, and professional podiatric care may be required to help relieve your discomfort. If you have not exercised in a long time, consult your podiatric physician before starting a new exercise program. Begin an exercise program slowly. Don't go too far or too fast. Purchase and maintain good shoes and replace them regularly. Stretch each foot and achilles tendon before and after exercise. Avoid uneven walking surfaces or stepping on rocks as much as possible. Avoid going barefoot on hard surfaces. Vary the incline on a treadmill during exercise. Nobody walks uphill all the time. If it hurts, stop. Don't try to "work through the pain." Your podiatric physician/surgeon has been trained specifically and extensively in the diagnosis and treatment of all manner of foot conditions. This training encompasses all of the intricately related systems and structures of the foot and lower leg including neurological, circulatory, skin, and the musculoskeletal system, which includes bones, joints, ligaments, tendons, muscles, and nerves.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Prevention
Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities.
Living With Achilles Tendonitis
Overview
 Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Causes
The causes of Achilles tendonitis all appear to be related to excessive stress being transmitted through the tendon. Weak calf muscles, poor ankle range of motion, and excessive pronation have all been connected with the development of Achilles problems.The upshot is that all of these factors, plus training volume and so on, result in damage to the tendon. Much like a bungee cord is made up of tiny strands of rubber aligned together, tendons are comprised of small fiber-like proteins called collagen. Pain in the Achilles tendon is a result of damage to the collagen. Because of this, treatment options should start with ways to address this.
Symptoms
Symptoms of Achilles tendonitis include, pain in the back of the heel, difficulty walking, sometimes the pain makes walking impossible, swelling, tenderness and warmth of the Achilles tendon. Achilles tendonitis is graded according to how severe it is, mild - pain in the Achilles tendon during a particular activity (such as running) or shortly after. Moderate - the Achilles tendon may swell. In some cases, a hard lump (nodule) may form in the tendon. Severe - any type of activity that involves weight bearing causes pain of the Achilles tendon. Very occasionally, the Achilles tendon may rupture (tear). When an Achilles tendon ruptures, it is said to feel like a hard whack on the heel.
Diagnosis
A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition.
Nonsurgical Treatment
Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs): Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy. Surgery may also be used in the treatment of Achilles tendinosis and paratenonitis. In paratenonitis, fibrotic adhesions and nodules are excised, freeing up the tendon. Longitudinal tenotomies may be performed to decompress the tendon. Satisfactory results have been obtained in 75-100% of cases. In tendinosis, in addition to the above procedures, the degenerated portions of the tendon and any osteophytes are excised. Haglund?s deformity, if present, is removed. If the remaining tendon is too thin and weak, the plantaris or flexor hallucis longus tendon can be weaved through the Achilles tendon to provide more strength. The outcome is generally less favorable than it is in paratenonitis surgery.

Surgical Treatment
Your doctor may recommend surgery if, after around six months, other treatments haven?t worked and your symptoms are having an impact on your day-to-day life. Surgery involves removing damaged areas of your tendon and repairing them.
Prevention
Warm up slowly by running at least one minute per mile slower than your usual pace for the first mile. Running backwards during your first mile is also a very effective way to warm up the Achilles, because doing so produces a gentle eccentric load that acts to strengthen the tendon. Runners should also avoid making sudden changes in mileage, and they should be particularly careful when wearing racing flats, as these shoes produce very rapid rates of pronation that increase the risk of Achilles tendon injury. If you have a tendency to be stiff, spend extra time stretching. If you?re overly flexible, perform eccentric load exercises preventively. Lastly, it is always important to control biomechanical alignment issues, either with proper running shoes and if necessary, stock or custom orthotics.
Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Causes
The causes of Achilles tendonitis all appear to be related to excessive stress being transmitted through the tendon. Weak calf muscles, poor ankle range of motion, and excessive pronation have all been connected with the development of Achilles problems.The upshot is that all of these factors, plus training volume and so on, result in damage to the tendon. Much like a bungee cord is made up of tiny strands of rubber aligned together, tendons are comprised of small fiber-like proteins called collagen. Pain in the Achilles tendon is a result of damage to the collagen. Because of this, treatment options should start with ways to address this.
Symptoms
Symptoms of Achilles tendonitis include, pain in the back of the heel, difficulty walking, sometimes the pain makes walking impossible, swelling, tenderness and warmth of the Achilles tendon. Achilles tendonitis is graded according to how severe it is, mild - pain in the Achilles tendon during a particular activity (such as running) or shortly after. Moderate - the Achilles tendon may swell. In some cases, a hard lump (nodule) may form in the tendon. Severe - any type of activity that involves weight bearing causes pain of the Achilles tendon. Very occasionally, the Achilles tendon may rupture (tear). When an Achilles tendon ruptures, it is said to feel like a hard whack on the heel.
Diagnosis
A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition.
Nonsurgical Treatment
Conservative management of Achilles tendinosis and paratenonitis includes the following. Physical therapy. Eccentric exercises are the cornerstone of strengthening treatment, with most patients achieving 60-90% pain relief. Orthotic therapy in Achilles tendinosis consists of the use of heel lifts. Nonsteroidal anti-inflammatory drugs (NSAIDs): Tendinosis tends to be less responsive than paratenonitis to NSAIDs. Steroid injections. Although these provide short-term relief of painful symptoms, there is concern that they can weaken the tendon, leading to rupture. Vessel sclerosis. Platelet-rich plasma injections. Nitric oxide. Shock-wave therapy. Surgery may also be used in the treatment of Achilles tendinosis and paratenonitis. In paratenonitis, fibrotic adhesions and nodules are excised, freeing up the tendon. Longitudinal tenotomies may be performed to decompress the tendon. Satisfactory results have been obtained in 75-100% of cases. In tendinosis, in addition to the above procedures, the degenerated portions of the tendon and any osteophytes are excised. Haglund?s deformity, if present, is removed. If the remaining tendon is too thin and weak, the plantaris or flexor hallucis longus tendon can be weaved through the Achilles tendon to provide more strength. The outcome is generally less favorable than it is in paratenonitis surgery.
Surgical Treatment
Your doctor may recommend surgery if, after around six months, other treatments haven?t worked and your symptoms are having an impact on your day-to-day life. Surgery involves removing damaged areas of your tendon and repairing them.
Prevention
Warm up slowly by running at least one minute per mile slower than your usual pace for the first mile. Running backwards during your first mile is also a very effective way to warm up the Achilles, because doing so produces a gentle eccentric load that acts to strengthen the tendon. Runners should also avoid making sudden changes in mileage, and they should be particularly careful when wearing racing flats, as these shoes produce very rapid rates of pronation that increase the risk of Achilles tendon injury. If you have a tendency to be stiff, spend extra time stretching. If you?re overly flexible, perform eccentric load exercises preventively. Lastly, it is always important to control biomechanical alignment issues, either with proper running shoes and if necessary, stock or custom orthotics.
What Exactly Causes Heel Pain

Overview
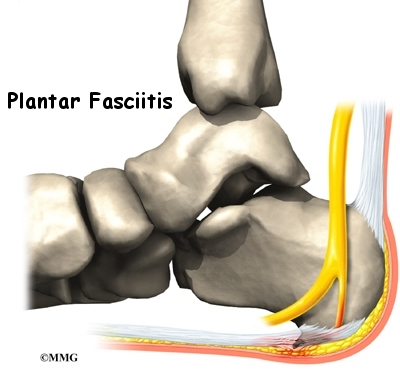
Heel pain is most often caused by plantar fasciitis, a condition that is sometimes also called heel spur syndrome when a spur is present. Heel pain may also be due to other causes, such as a stress fracture, tendonitis, arthritis, nerve irritation, or, rarely, a cyst. Because there are several potential causes, it is important to have heel pain properly diagnosed. A foot and ankle surgeon is able to distinguish between all the possibilities and determine the underlying source of your heel pain. Plantar fasciitis is an inflammation of the band of tissue (the plantar fascia) that extends from the heel to the toes. In this condition, the fascia first becomes irritated and then inflamed, resulting in heel pain.
Causes
When the foot moves, the plantar fascia stretches and contracts. Plantar fasciitis is caused by the repetitive overstretching of the plantar fascia. If the tension on the plantar fascia is too great, this overstretching causes small tears in the plantar fascia. This in turn causes the plantar fascia to become inflamed and painful. Factors that contribute to the development of plantar fasciitis include having very high arches or flat feet, gender, while anyone can develop plantar fasciitis, it tends to occur more commonly in women, exercises such as running, walking and dancing, particularly if the calf muscles are tight. Activities or occupations that involve walking or standing for long periods of time, particularly on hard surfaces, wearing high heeled shoes or shoes that do not offer adequate arch support and cushioning, being overweight, additional weight increases the tension on the plantar fascia, poor biomechanics, extra tension is placed on the plantar fascia if weight is not spread evenly when standing, walking or running. Some cases of plantar fasciitis may be linked to underlying diseases that cause arthritis, such as ankylosing spondylitis.
Symptoms
Symptoms of plantar fasciitis include pain in the heel of the foot. Some people complain of a sharp stabbing pain especially with walking. Others describe the pain as a dull ache after prolonged standing. The pain of plantar fasciitis is often worst in the morning or following activity.
Diagnosis
Your doctor may look at your feet and watch the way you stand, walk and exercise. He can also ask you questions about your health history, including illnesses and injuries that you had in your past. The symptoms you have such as the pain location or when does your foot hurts most. Your activity routine such as your job, exercise habits and physical activities preformed. Your doctor may decide to use an X-ray of your foot to detect bones problems. MRI or ultrasound can also be used as further investigation of the foot condition.
Non Surgical Treatment
A doctor may prescribe anti-inflammatory medication such as ibuprofen to help reduce pain and inflammation. Electrotherapy such as ultrasound or laser may also help with symptoms. An X-ray may be taken to see if there is any bone growth or calcification, known as a heel spur but this is not necessarily a cause of pain. Deep tissue sports massage techniques can reduce the tension in and stretch the plantar fascia and the calf muscles. Extracorporeal shock wave therapy has been known to be successful and a corticosteroid injection is also an option.

Surgical Treatment
In very rare cases plantar fascia surgery is suggested, as a last resort. In this case the surgeon makes an incision into the ligament, partially cutting the plantar fascia to release it. If a heel spur is present, the surgeon will remove it. Plantar Fasciitis surgery should always be considered the last resort when all the conventional treatment methods have failed to succeed. Endoscopic plantar fasciotomy (EPF) is a form of surgery whereby two incisions are made around the heel and the ligament is being detached from the heel bone allowing the new ligament to develop in the same place. In some cases the surgeon may decide to remove the heel spur itself, if present. Just like any type of surgery, Plantar Fascia surgery comes with certain risks and side effects. For example, the arch of the foot may drop and become weak. Wearing an arch support after surgery is therefore recommended. Heel spur surgeries may also do some damage to veins and arteries of your foot that allow blood supply in the area. This will increase the time of recovery.
Prevention
Stretching the plantar fascia and the calf muscle area can help to prevent inflammation. Slowly increasing the amount or intensity of athletic activities by graded progression can also help to prevent injury. Recommended Stretches: Taking a lunge position with the injured foot behind and keeping your heels flat on the floor, lean into a wall and bend the knees. A stretch should be felt in the sole and in the Achilles tendon area. Hold the stretch for 20-30 seconds. Also try this stretch with the back leg straight.
What May Cause Painful Heel

Overview
Heel pain is a common foot condition. It's usually felt as an intense pain when using the affected heel. Heel pain usually builds up gradually and gets worse over time. The pain is often severe and occurs when you place weight on the heel. In most cases, only one heel is affected, although estimates suggest that around a third of people have pain in both heels. The pain is usually worse first thing in the morning, or when you first take a step after a period of inactivity. Walking usually improves the pain, but it often gets worse again after walking or standing for a long time. Some people may limp or develop an abnormal walking style as they try to avoid placing weight on the affected heel.
Causes
The plantar fascia is designed to absorb the high stresses and strains we place on our feet. But, sometimes, too much pressure damages or tears the tissues. The body's natural response to injury is inflammation, which results in the heel pain and stiffness of plantar fasciitis.
Symptoms
The main symptom of plantar fasciitis is heel pain when you walk. You may also feel pain when you stand and possibly even when you are resting. This pain typically occurs first thing in the morning after you get out of bed, when your foot is placed flat on the floor. The pain occurs because you are stretching the plantar fascia. The pain usually lessens with more walking, but you may have it again after periods of rest. You may feel no pain when you are sleeping because the position of your feet during rest allows the fascia to shorten and relax.
Diagnosis
The health care provider will perform a physical exam. This may show tenderness on the bottom of your foot, flat feet or high arches, mild foot swelling or redness, stiffness or tightness of the arch in the bottom of your foot. X-rays may be taken to rule out other problems.
Non Surgical Treatment
Usually, the pain will ease in time. 'Fascia' tissue, like 'ligament' tissue, heals quite slowly. It may take several months or more to go. However, the following treatments may help to speed recovery. A combination of different treatments may help. Collectively, these initial treatments are known as 'conservative' treatments for plantar fasciitis. Rest your foot. This should be done as much as possible. Avoid running, excess walking or standing, and undue stretching of your sole. Gentle walking and exercises described below are fine. Footwear. Do not walk barefoot on hard surfaces. Choose shoes with cushioned heels and a good arch support. A laced sports shoe rather than an open sandal is probably best. Avoid old or worn shoes that may not give a good cushion to your heel. Heel pads and arch supports. You can buy various pads and shoe inserts to cushion the heel and support the arch of your foot. These work best if you put them in your shoes at all times. The aim is to raise your heel by about 1 cm. If your heel is tender, cut a small hole in the heel pad at the site of the tender spot. This means that the tender part of your heel will not touch anything inside your shoe. Place the inserts/pads in both shoes, even if you only have pain in one foot. Pain relief. Painkillers such as paracetamol will often ease the pain. Sometimes anti-inflammatory medicines such as ibuprofen are useful. These are painkillers but also reduce inflammation and may work better than ordinary painkillers. Some people find that rubbing a cream or gel that contains an anti-inflammatory medicine on to their heel is helpful. An ice pack (such as a bag of frozen peas wrapped in a tea towel) held to your foot for 15-20 minutes may also help to relieve pain. Exercises. Regular, gentle stretching of your Achilles tendon and plantar fascia may help to ease your symptoms. This is because most people with plantar fasciitis have a slight tightness of their Achilles tendon. If this is the case, it tends to pull at the back of your heel and has a knock-on effect of keeping your plantar fascia tight. Also, when you are asleep overnight, your plantar fascia tends to tighten up (which is why it is usually most painful first thing in the morning). The aim of these exercises is to loosen up the tendons and fascia gently above and below your heel. Your doctor may refer you to a physiotherapist for exercise guidance.

Surgical Treatment
Plantar fasciotomy is often considered after conservative treatment has failed to resolve the issue after six months and is viewed as a last resort. Minimally invasive and endoscopic approaches to plantar fasciotomy exist but require a specialist who is familiar with certain equipment. Heel spur removal during plantar fasciotomy has not been found to improve the surgical outcome. Plantar heel pain may occur for multiple reasons and release of the lateral plantar nerve branch may be performed alongside the plantar fasciotomy in select cases. Possible complications of plantar fasciotomy include nerve injury, instability of the medial longitudinal arch of the foot, fracture of the calcaneus, prolonged recovery time, infection, rupture of the plantar fascia, and failure to improve the pain. Coblation (TOPAZ) surgery has recently been proposed as alternative surgical approaches for the treatment of recalcitrant plantar fasciitis.
What Leads To Plantar Fasciitis And The Ways To End It

Overview
Plantar fasciitis is one of the most common explanations of heel pain. It is caused by inflammation to the thick band that connects the toes to the heel bone, called the plantar fascia, which runs across the bottom of your foot. The condition is most commonly seen in runners, pregnant women, overweight people, and individuals who wear inadequately supporting shoes. Plantar fasciitis typically affects people between the ages of 40 and 70. Plantar fasciitis commonly causes a stabbing pain in the heel of the foot, which is worse during the first few steps of the day after awakening. As you continue to walk on the affected foot, the pain gradually lessens. Usually, only one foot is affected, but it can occur in both feet simultaneously. To diagnose plantar fasciitis, your doctor will physically examine your foot.
Causes
Your plantar fascia (fay-sha) supports the arch of your foot as you run or walk. It is a thick, inelastic, fibrous band that starts in your heel, runs along the bottom of your foot, and spreads out to your toes. Plantar fasciitis is an inflammation of this fibrous band. If you are female or have a job that requires a lot of walking or standing on hard surfaces you are more at risk for plantar fasciitis. Additional causes include Being overweight, Having flat feet or high arches, Wearing shoes with poor support, Walking or running for exercise, Tight calf muscles that limit how far you can flex your ankles, Running on soft terrain, Increase in activity level, Genetic predisposition.
Symptoms
The most common symptom is pain and stiffness in the bottom of the heel. The heel pain may be dull or sharp. The bottom of the foot may also ache or burn. The pain is often worse in the morning when you take your first steps, after standing or sitting for awhile, when climbing stairs, after intense activity. The pain may develop slowly over time, or come on suddenly after intense activity.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
The following recommendations are appropriate. Wear shoes with adequate arch support and cushioned heels; discard old running shoes and wear new ones; rotate work shoes daily. Avoid long periods of standing. Lose weight. Stretch the plantar fascia and warm up the lower extremity before participating in exercise. For increased flexibility, stretch the plantar fascia and the calf after exercise. Do not exercise on hard surfaces. Avoid walking barefooted on hard surfaces. Avoid high-impact sports that require a great deal of jumping (eg, aerobics and volleyball). Apply ice for 20 minutes after repetitive impact-loading activities and at the end of the day. Limit repetitive impact-loading activities such as running to every other day, and consider rest or cross-training for nonrunning days.
Surgical Treatment
Most studies indicate that 95% of those afflicted with plantar fasciitis are able to relieve their heel pain with nonsurgical treatments. If you are one of the few people whose symptoms don't improve with other treatments, your doctor may recommend plantar fascia release surgery. Plantar fascia release involves cutting part of the plantar fascia ligament in order to release the tension and relieve the inflammation of the ligament. Overall, the success rate of surgical release is 70 to 90 percent in patients with plantar fasciitis. While the success rate is very high following surgery, one should be aware that there is often a prolonged postoperative period of discomfort similar to the discomfort experienced prior to surgery. This pain usually will abate within 2-3 months. One should always be sure to understand all the risks associated with any surgery they are considering.